
[歩行に違和感を覚えたことはありませんか?][BOC-ATC対策]トレンデレンブルグ歩行について

BOC-ATC対策用英文ノートは後半です。
トレンデレンブルグ歩行とは
トレンデレンブルグ歩行とは、片側の股関節外転筋、特に中殿筋や小殿筋が弱くなることで起こる独特な歩き方を指します。
これらの筋肉が弱まると、歩くときに体重を支えるのが難しくなり、以下の特徴が現れます。

通常の歩行と異常な歩行の違い
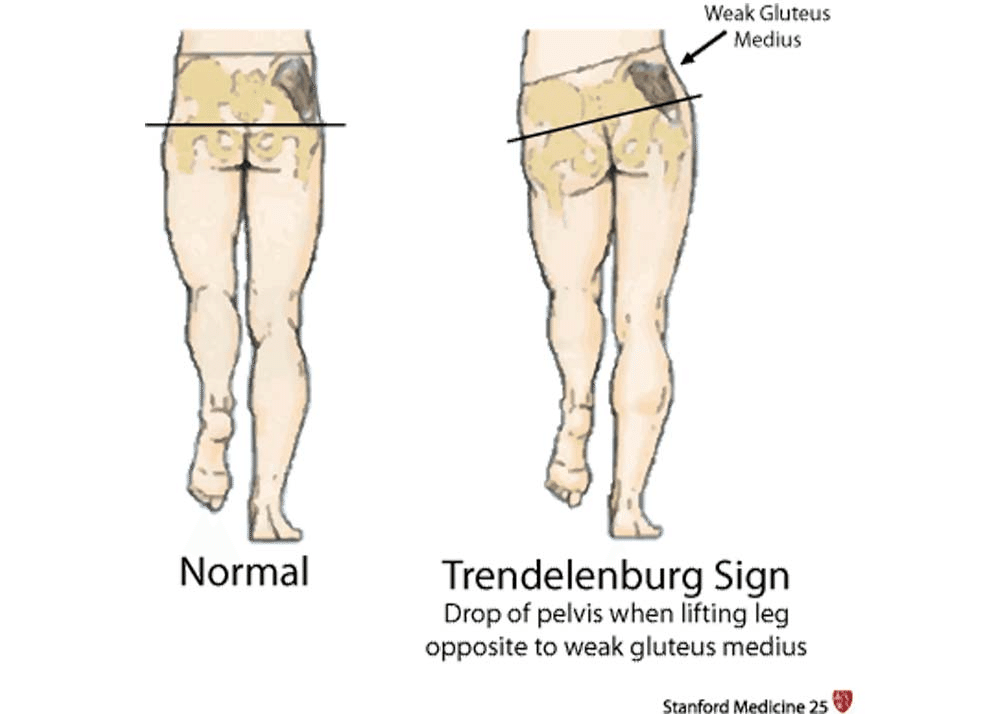
普通の歩行では、片方の脚が地面に着いている間、その脚が体全体の体重を支えます。
このとき、骨盤は体重を支えている側で安定し、反対側が少し上がるのが正常です。
しかし、トレンデレンブルグ歩行では、股関節外転筋が弱くなっているため、骨盤が体重を支えていない側に下がるようになります。
この状態を補うため、患者さんは上半身を患っている側に傾けます。
これにより、重心が立っている脚のほうに移動し、骨盤が大きく傾くのを防ぎます。
トレンデレンブルグ歩行の主な原因
トレンデレンブルグ歩行が起こる原因は、大きく3つに分けられます。
神経の問題:
上殿神経の損傷や腰椎神経根症が含まれます。(L4-S1)
先天性の問題:
股関節形成不全や先天性股関節脱臼などが原因となります。
手術後の合併症:
人工股関節置換術後に発生することがあります。
診断方法
トレンデレンブルグ歩行を診断するために、トレンデレンブルグサインというテストが一般的です。
このテストでは、患者さんが片脚立ちをしたときに、上がっている脚側の骨盤が下がるかどうかを確認します。
もし骨盤が下がれば、(つまり、上記で述べた独特・異常な歩行姿勢が見られれば)このテストは陽性と判断されます。
さらに、X線検査も行い、骨や関節の状態を詳しく調べた方が良いでしょう。
これにより、原因となっている病気や異常が特定されることがあります。
治療方法
トレンデレンブルグ歩行の治療は、原因によって異なります。
以下に代表的な治療方法を挙げます。
手術による治療
小児の場合:
股関節形成不全に対しては、観血的整復術やSalter骨盤骨切り術が効果的と言われています。
成人の場合:
骨盤支持骨切り術が歩行能力の改善に役立つとされています。
理学療法
理学療法では、基本的に股関節外転筋を強化することがゴールドスタンダードです。
基本的な運動:
横向きに寝た状態で股関節外転運動を行います。(クラムシェルやサイドレッグレイズなど)
徐々に負荷を増やして筋力を強化します。

応用的な運動:
クローズドチェーン運動(足を床に固定して行う運動ースクワットなど)や側方ステップアップ、バランス運動が効果的です。
バイオフィードバックを用いた治療
最近では、EMG(筋電図)バイオフィードバックという方法が注目されています。
この治療では、中殿筋の活動を監視し、異常な動きがあれば音などで警告します。これにより筋肉の活動を自分自身で意識・感知しやすくります。
家庭用の装置を使った研究では、2ヶ月後に正常な歩行をほぼ回復したという報告もあります。

鏡を使った治療
鏡を使って自分の歩き方を確認する方法も効果的です。
患者さんは自分の姿勢を見ながら、セラピストの指導のもとで正しい歩行姿勢の確認を行います。
注意点と長期的な影響
トレンデレンブルグ歩行を放置すると、股関節や膝関節に負担がかかり、関節症や早期の関節摩耗につながることがあります。
そのため、早期の診断と適切な治療が非常に重要です。
また、リハビリを継続することで、多くの場合、歩行能力の改善が期待できます。治療チームは、患者さんの年齢や生活環境に合わせたプログラムを作成することが理想的でしょう。
患者さん自身も、自主的にトレーニングや適度な運動を続けることが大切です。
理学療法士のアドバイスを受けながら、日常的に適切な運動を行うことで、治療効果がより高まります。
まとめ
トレンデレンブルグ歩行は、股関節外転筋(主に中臀筋)の弱化によって起こる歩行異常ですが、原因に応じた治療やリハビリテーションで改善が可能です。
医療チームと患者さんが協力して取り組むことで、日常生活の質を向上させることがでるでしょう。
もし歩行時に違和感を感じた場合は、早めに専門医に相談することをお勧めします。
Definition/ Description:
Trendelenburg gait is characterized by these key features:
A condition where hip abductor muscles, particularly the gluteal muscles (Glute med), become weak on one side due to superior gluteal nerve damage or L5 spine injury.
In normal walking, each leg supports half the body weight during stance phase, causing the pelvis to tilt downward on the weight-bearing side and upward on the non-weight-bearing side.
When hip abductors are weak, the pelvis abnormally drops on the non-weight-bearing side instead of lifting upward.
To compensate, people lean their upper body away from the weak hip, shifting their center of gravity over the standing leg to minimize pelvic drop.
This condition mainly affects a person's ability to support their body weight on the weak side while walking.
Clinically Relevent Anatomy
Primary hip abductors: Gluteus medius and minimus muscles - prevent pelvic drop and maintain pelvic stability
Superior gluteal nerve: Originates from L4-S1 nerve roots, exits through sciatic notch, innervates:
Hip joint
Gluteus medius and minimus muscles
Tensor fascia lata
Epidemiology
Biomechanical basis: Hip joint acts as class 3 lever system - pathology in fulcrum, load, effort, or lever causes Trendelenburg gait
Fulcrum failure conditions:
Osteonecrosis of hip
Legg-Calve-Perthes disease
Developmental hip dysplasia
Chronic hip dislocations (trauma/infection)
Lever failure conditions:
Greater trochanteric avulsion
Femoral neck non-union
Coxa vara
Effort failure conditions:
Poliomyelitis
L5 radiculopathy
Superior gluteal nerve damage
Gluteal muscle problems (tendinitis/abscess)
Post hip replacement
Additional causes:
Neuronal injury (nerve entrapment/iatrogenic)
Congenital conditions (mechanical disadvantage)
Post-surgical complications
Muscular dystrophy
Hemiplegic cerebral palsy
Primary cause: Paralysis or weakness of hip abductors, often from superior gluteal nerve injury (entrapment or iatrogenic).
Developmental conditions: Occurs in hip dysplasia, congenital hip dislocation, coxa vara/valga, and Legg-Calvé-Perthes disease - muscles normal but mechanically disadvantaged.
Post-surgical cases: Common after hip replacement and femoral fixation due to gluteus medius dissection, typically resolves with healing.
Additional causes: Can present in muscular dystrophy and hemiplegic cerebral palsy.
Exam
The Trendelenburg sign determines the integrity of hip abductor muscle function.
Medical Management
Surgical interventions: Open reduction and Salter innominate osteotomy for young children with hip dysplasia, pelvic support osteotomies for congenital dislocations
Osteopathic Manipulative Treatment (OMT) improves gait parameters in somatic dysfunctions
Physical Therapy Management
Core exercises:
Side-lying hip abduction with progressive resistance
Functional closed-chain exercises
Lateral step-ups
Balance exercises
General hip muscle strengthening
Biofeedback techniques:
EMG biofeedback: Reduces gait deviation by 29°, improves stride length and speed
Two-channel EMG home training device: Shows significant improvement after two months
Wall mirror feedback: Helps correct posture and range of motion
Treatment goals focus on preventing secondary complications like arthritis and premature joint wear through proper rehabilitation and strengthening.